
Amy Garcia, MD. Albuquerque, New Mexico, USA
The FIGO abnormal uterine bleeding (AUB) category of myomas and subclassification of submucous myomas as types 0, 1 and 2 is used to diagnose and describe myomas within the uterine cavity. There are several imaging modalities available to the gynecologist for submucous myoma diagnosis.
Transvaginal Ultrasound
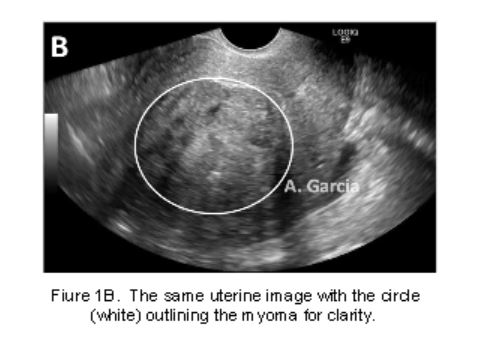
A 2-dimensional transvaginal ultrasound (2DTVUS) is generally the first-line diagnostic procedure for evaluating AUB for most women.(Figura 1) It is a safe and cost-effective tool which is fully utilizable in the office. Initial 2DTVUS findings of any endometrial abnormality, presence of fibroids or suspicion of adenomyosis warrants evaluation of the cavity with hysteroscopy.
Power Doppler is more sensitive than color Doppler for the detection of blood flow but provides no information about the direction of flow. When added to gray scale TVUS, circular vessel flow pattern correlates with a high level of specificity for the diagnosis of submucous myomas compared to HS (sensitivity 72.2%, specificity 100%, PPV 100% and NPV of 88.9%). There are differences, however, in diagnostic accuracy of intracavitary pathology between 2DTVUS, saline infusion sonography (SIS) and hysteroscopy. In a large systematic review of studies comparing these three imaging techniques, both SIS and HS identify intrauterine pathology better than 2DTVUS.

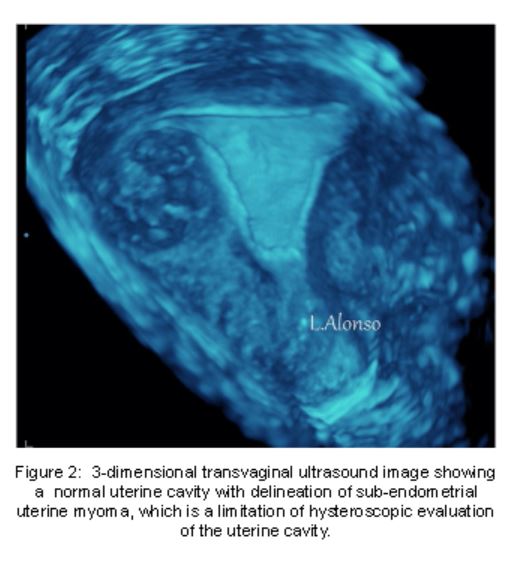

With 3DTVUS imaging, uterine cavity evaluation is enhanced above gray scale 2DTVUS. The 3D scan simultaneously displays three perpendicular image planes creating a detailed image construction of surface detail. One advantage of 3DTVUS over HS is the evaluation of sub-endometrial regions of the uterus as well as the endometrial cavity (Figure 2) . Hysteroscopy, however, still more accurately identifies submucous myomas.
Saline Infusion Sonography
Saline infusion sonography is well tolerated by patients and performed when endometrium on TVUS is abnormal. A small catheter is placed first into the uterine cavity via the cervical canal, and a small amount of saline is instilled via syringe into the uterine cavity during a TVUS procedure. The saline provides a contrast medium so focal lesions of the endometrium are identifiable more readily than for TVUS alone. Figure 3 Compared to hysteroscopy, SIS is not as good at identification of submucous myomas.

A Cochran Systematic Review (meta-analysis) comparing studies of 2DSIS versus 3DSIS concluded that there is no statistically significant difference between 2DSIS and 3DSIS for diagnostic accuracy in the evaluation of the uterine cavity.[5] However, a recent comparison of 3DSIS versus HS for the classification of submucous myomas found agreement between the two with 92% for type 0, 92% for type 1 and 75% for type 2 with hysteroscopy remaining superior. As with 2D and 3D TVUS, the SIS also requires fundamental skills in ultrasound interpretation.
Hysteroscopy
Hysteroscopy is essential in the evaluation of AUB and especially in the office environment where it is cost effective and well tolerated by patients. Dr. Linda Bradley, a preeminent leader in hysteroscopic surgical education has coined the phrase, “My hysteroscope is my stethoscope.” As gynecologists, we should be as adept at using a hysteroscope in the office as the cardiologist is at using a stethoscope. Hysteroscopy remains the gold standard for evaluation of the uterine cavity as it improves our diagnostic capabilities over blinded procedures such as endometrial biopsy and dilation and curettage and has consistently shown superiority over 2D and 3D sonography modalities for identification of intracavitary lesions. Figure 5, 6, 7




Magnetic Resonance Imaging
A study evaluating preoperative TVUS, SIS, HS and magnetic resonance imaging (MRI) showed that submucous myomas were best identified with MRI (100% sensitivity, 91% specificity). Also, MRI evaluates submucous, intramural and subserosal myomas, helping to define preoperative myoma mapping Figure 8,9. However, MRI is a more expensive imaging technique than sonography and office hysteroscopy and may not be readily available because of prohibitive cost and is not accessible in the office.
Conclusion
Diagnosis of submucous myomas and pre-operative decisions often utilize a combination of imaging such as sonography and hysteroscopy to assess myoma morphologic qualities, size, number, position with the cavity and subclassification of type to determine the degree of difficulty for removal and the likelihood of success. Use of MRI has distinct advantages beyond cavity evaluation for myoma mapping of uterine myomas prior to myomectomy.

0 comments on “Evaluation of the Uterine Cavity and Diagnosis of Submucous Myomas”