

The cesarean section rate is alarmingly increasing in recent years in developed countries, this has been associated with an increase in the economic expense derived from the surgical intervention and on the other hand the appearance of new problems derived from the cesarean section itself, which may be both obstetric and gynecological in nature.
The most frequently documented in the literature are poor obstetric consequences in subsequent pregnancies after cesarean section, being well recognized the correlation between a previous cesarean section and the risk of developing placenta previa, placental accreta, implantation of pregnancy at the level of the cesarean scar and uterine rupture. Among future gynecological problems described in patients undergoing cesarean section are abnormal uterine bleeding, dyspareunia and abdominal pain.
When performing a pelvic ultrasound in patients with history of cesarean section, it is frequent to find a hypoecogenic area, generally triangular with the vertex directed towards the bladder of different sizes, at the level of the previous caesarean section scar. This ultrasound image, defined as an “Isthmocele”. It is a uterine wall sac-like structure located in the lower uterine wall, just in the area of the scar of a previous cesarean section.
The importance of the isthmocele lies, on the one hand, in its correlation to abnormal uterine bleeding that is usually post-menstrual, and on the other hand in its relationship with secondary infertility. Regarding to the abnormal bleeding, the main cause is that the isthmocele acts as a reservoir that hinders the flow of the menstrual blood; In addition, there is minimal “in situ” blood production derived from the increase in local vascularization at the level of the base of the isthmocele and local alteration of uterine contractility. Regarding the correlation with secondary infertility, the persistence of menstrual flow at the cervical level has a negative impact on sperm transport as well as implantation.
Several mechanisms to explain the isthmocele formation are considered. One is the difference in thickness between the anterior and posterior segments of the hysterotomy, another the different types of suture material used to close the hysterotomy. It seems that the more ischemic areas are created, the greater the possibility of developing an isthmocele, this leads to consider whether the use of 2 layers closure technique of the hysterotomy increases the risk of isthmocele formation.
The diagnosis of isthmocele is based on clinical signs and complementary tests such as ultrasound, hysterosonography and/or hysteroscopy. The ultrasound shows the presence of an hypoecogenic area, generally of triangular shape, located at the isthmic level with the vertex of it directed towards the bladder (3). This isthmocele is echographically more evident if ultrasound is performed during the postmenstrual phase, since blood accumulation facilitates the visualization as an ecogenic area. The measures that are usually carried out in this ecogenic area, are the ones to measure their area, following the formula (base x height / 2), classifying the
istmoceles according to the result in 3 degrees, grade 1 when the area is less than 15 mm², Grade 2 between 16 and 24 mm² and grade 3 when it is greater than 25 mm².

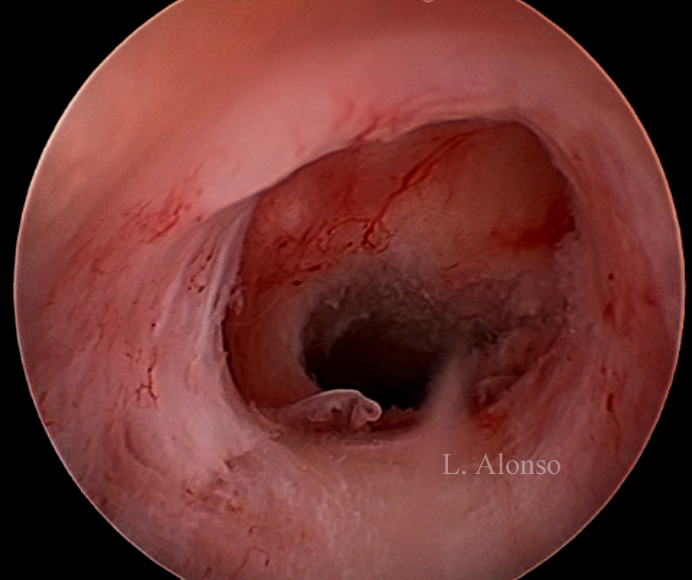
Hysterosonography enhance visualization of the isthmocele even when there is no blood accumulation inside of it. Hysteroscopy is the “Gold Standard” technique for the diagnosis of isthmocele. Hysteroscopy allows direct visualization of the anterior and posterior borders of the isthmocele that some authors define as an anterior and a posterior arch, the isthmocele is actually the area contained between these two arches.
There are several proposed treatments aimed at resolving the symptomatology associated with the isthmocele, especially bleeding and secondary infertility. The use of hormonal treatment has shown a decrease in the duration of post-menstrual bleeding and an improvement with respect to the associated symptomatology, although they do not eliminate the symptoms and have been less effective than surgical treatment. Some experts prefer to the laparoscopic (4) and even transvaginal route for the surgical treatment of the scar dehiscence of a previous cesarean section.
The hysteroscopic repair of a cesarean scar is frequently referred as Isthmoplasty. The surgical technique first described by Fernandez in 1996 at the 25th annual meeting of the AAGL (5), consists of remodeling the sac “flattening” the area of the isthmocele from the lower arch to the external cervical os. The surgical procedure must be performed extremely carefully and very superficially, taking into account that the dome of the isthmocele is in close contact with the bladder
and the lateral areas of the defect with the uterine arteries (1). In addition to carrying out the resection of the fibrotic tissue, Fabres favors the treatment of the tissue at the base of the defect by means of the local fulguration of the dilated vessels as well as the inflammatory tissue, responsible for the “in situ” blood production.
The latest studies show that the surgical treatment of the isthmocele eliminates the symptoms of postmenstrual spotting in the vast majority of patients, it is also important to note that after surgery, some patients restore their fertility, obtaining in these patients pregnancy in the first 6-12 months after surgical correction (6).
CONCLUSIONS
The surgical treatment of isthmocele aims to avoid retention of menstrual blood at the level of the defect, eliminating post-menstrual spotting pattern and its consequences. The hysteroscopic approach is a symptomatic treatment, while laparoscopic or vaginal treatment aims to repair the defect, so are considered a restorative treatment. As a general rule, it is accepted that in cases in which the residual myometrium thickness at the level of the isthmocele is greater than 3 mm, the hysteroscopic approach is an adequate and safe option. However, if the endometrial thickness at this level is less than 3 mm, the laparoscopic approach should be preferred because of the risk of uterine perforation and allows to restore the uterine wall at that level. (7)
After surgical treatment, a new questions arise, such as whether a spontaneous vaginal delivery is safe after the completion of the isthmoplasty. The recommendation of the Global Congress of Hysteroscopy Research Committee is the to perform an elective cesarean section no later than week 38 of gestation due to the risk of uterine rupture (7)
It is important to bear in mind that post-menstrual bleeding in patients with a previous caesarean section may be related to the presence of an isthmocele and that they can also cause secondary infertility. It is also important to remember that the only treatment of this condition is surgical and that hormonal treatments do not solve the problem.

0 comments on “Istmocele: overview”